The K-level scale has shaped amputees’ lives for three decades. Does the system still serve us? Or is it time for something better?
 Image a life defined by a number. Not your age, not your achievements, but a cold, clinical classification that dictates whether you can chase your grandchildren, return to work, or simply walk without fear of falling.
Image a life defined by a number. Not your age, not your achievements, but a cold, clinical classification that dictates whether you can chase your grandchildren, return to work, or simply walk without fear of falling.
For 30 years, the K-level system has held that power over amputees. A relic from 1995, long before microprocessor knees and other bionic advancements were common, this system reduces human potential to a single digit between 0 and 4. That number packs in a lot of complexity, but it doesn’t always capture every nuance of a person’s circumstances. As a result, K-levels often keep amputees from getting the outcomes they want.
Take Jenna. Before limb loss she was incredibly energetic—a runner, a hiker, the kind of person who never sat still for long. But after a serious leg injury, she spent years in and out of hospitals, enduring multiple limb-salvage surgeries that kept her from doing the things she used to live for. By the time she finally decided to amputate, Jenna had lost muscle, gained weight, and was struggling with chronic pain. She was not the same person she had been before.
When she got her K-level assessment, Jenna was rated a K2, meaning she was only considered capable of limited walking on flat surfaces. That rating didn’t reflect who she was before her medical challenges, nor who she aspired to be after recovering from amputation. It simply reflected a body that had spent years in survival mode.
Unfortunately, that K2 rating prevented Jenna from getting all the support she needed to recover fully and return to an active lifestyle. Insurers use K-levels to determine what type of prosthesis they’ll cover, and as a K2, Jenna would only qualify for a basic prosthesis that was unsuitable for hiking, running, climbing, or other demanding endeavors.
Like Jenna, most amputees don’t get classified when they’re at their strongest. We usually get classified when we’re at our weakest, when our bodies bear the full burden of surgeries, pain, forced idleness, and other stressors. Many of us have hit rock bottom at the very moment when we get assigned a K-level, which largely determines what technology we can afford, what quality of life we can look forward to, and even what type of person we can be.
That’s what happened to David, a construction worker whose identity revolved around his job. Strong and physically imposing, he prided himself on his ability to handle the toughest jobs and keep up with the hardiest crews. But after losing a limb in a workplace accident, he made slow progress in the initial rehabilitation phase, so when it came time to assign a K-level, David—who until recently had spent most days on his feet for demanding ten-hour shifts—was classified as a K2. His prosthetist believed he had K3 potential, but David’s insurance wouldn’t cover a device that would equip him to realize that objective.
The K2 classification trapped David in a cycle. His standard prosthesis held him back from rebuilding his strength. He grew frustrated and discouraged as his recovery plateaued; over time, he lost motivation and stopped trying so hard, believing no amount of effort would enable him to return to his job. David’s K-level threatened not only his livelihood but also his sense of identity. By limiting David to a prosthesis that didn’t fit his self-image, the K2 classification became a self-fulfilling prophecy.
Stories like David’s and Jenna’s aren’t uncommon. That’s why so many amputees and clinicians believe the K-level system is overdue for change. Can a framework created in 1995 still meet the needs of today’s amputees and prosthetists? Does it merely need to be tweaked, or is it time for a complete overhaul?
What K-Levels Are, and Why They Matter
The K-level system was introduced in 1995 as a way to categorize every amputee’s “functional potential.” Prosthetists use the number to gauge what mobility aids will best fit a patient’s needs, while Medicare and other insurance providers use K-levels to determine what technology is “medically necessary” to support an individual’s activities of daily living.
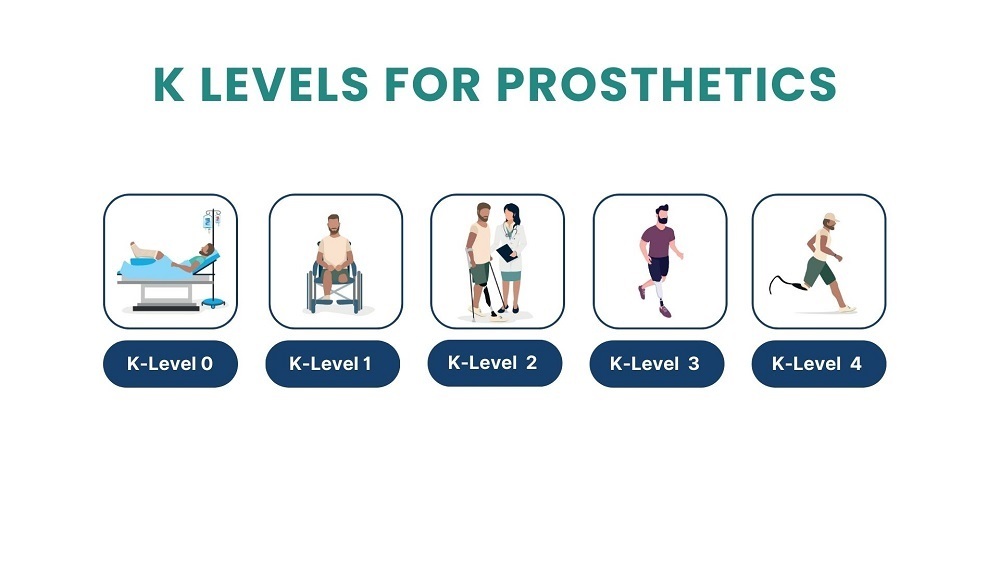
The levels, ranging from K0 to K4, indicate the predicted ability to function with and benefit from a prosthesis. A person receives a K0 rating if they lack the strength, stamina, and overall fitness to have a realistic hope of walking safely. K1 amputees are deemed capable of walking for limited distances at a fixed speed or cadence, primarily at home. The most common rating, K2, applies to people who can ambulate on a prosthesis for routine activities such as shopping, commuting to work, social outings, and similar tasks. At level K3, amputees can get coverage for advanced devices (including microprocessor ankles and knees) that support demanding work like David’s construction job, and vigorous recreation such as Jenna’s hiking and running. People in elite condition—competitive athletes, workout warriors, backcountry explorers—are classified as K4.
In theory, this system ensures that every amputee receives prosthetic devices they can comfortably use and maintain, and that help them regain pre-amputation levels of functional mobility. But in practice, K-levels often limit access to technology that could help people regain the lives they once had—or reach new goals they never thought possible.
These mismatches don’t only happen at the low end of the scale. K-levels can also create challenges for individuals deemed high-functioning. I’m an example of that. Perhaps I’m an outlier, but being assigned a high K-level actually diminished my quality of life. When I changed prosthetic clinics after moving to a new city, the care team fixated on my K4 classification and outfitted me with the most advanced suspension and foot technology available at the time. I was placed in a heavy vacuum suspension system paired with a substantial hydraulic ankle. But since I didn’t meet the weight requirement for this device, I couldn’t make the ankle articulate.
Moreover, this high-tech setup wasn’t compatible with my lifestyle. I find solace and joy in the outdoors, but the advanced leg was not built for navigating rough trails or the unpredictable terrain of nature. I yearned for a simpler, more adaptable foot, but my high-functioning label boxed me in, pushing me into a category I had no desire to occupy and that made it harder, not easier, for me to participate in the activities I loved.
My experience highlights what is perhaps the biggest flaw in the K-level system: a one-size-fits-all definition of “mobility” that fails to recognize individual preferences and lifestyle goals. Mobility isn’t just about what you can do; it’s about what you want to do and what brings you fulfillment. A system that ignores personal needs can be just as limiting as one that denies access altogether.
Four Flaws in the K-level System
To gauge the amputee community’s sentiment about K-levels, I conducted an informal poll among my 14,000 followers on social media. It wasn’t a scientific survey, but the results were emphatic: There was zero positive feedback. Not a single respondent felt the K-level system was serving them well. Instead, people unanimously viewed K-levels as a limiting, emotionally taxing system that left them feeling as if insurance companies dictate their lives.
The comments generally sorted themselves into four categories. First of all, K-levels are based on outdated notions of what prosthetic technology can do. They don’t account for microprocessor knees, powered ankles, specialized running blades, adjustable sockets, 3D printing, and other innovations that have emerged since 1995. Amputees and prosthetists now enjoy far more technological choices and combinations than they did 30 years ago, enabling them to select components that are targeted to specialized wants and needs. Yet the K-level system remains frozen in time, when the range of options was far narrower than it is today.
Second, K-level assessments occur when people are at their lowest point. Most people only undergo amputation after some combination of illness, infection, pain, immobility, and/or limb-salvage surgery. Those who suffer limb loss due to traumatic injury often face complex recoveries that involve multiple parts of the body. All too often, their K-level assessment happens when they’re at their weakest physically, mentally, and emotionally. This creates a flawed assessment. A person who has spent weeks or months bedridden may initially struggle to walk post-amputation, but that doesn’t mean they can’t become highly active once they regain strength. Their K-level assignment assumes their fitness potential is fixed, rather than something that can evolve with recovery.
Third, K-levels can shape amputees’ self-perceptions and take a psychological toll. The K-level system doesn’t just limit access to prosthetics—it can also limit belief in what’s possible. Being judged a K1 or K2 can feel like a life sentence, diminishing the hope that true mobility will ever be attainable. This “K-level destiny” effect can be deeply demoralizing, making amputees feel like their future has already been decided for them.
Finally, some evidence suggests that K-levels may unintentionally disadvantage certain types of patients. For example, senior amputees may get lower K-levels because of their age, even if they were highly active just before their amputation. Women generally have lower muscle mass than men, which makes them more prone to post-surgical weakness and may translate into lower K-levels. Amputees from minority and/or low-income communities often face barriers to basic healthcare, making it harder to demonstrate functional potential during a K-level assessment. More research is needed to establish the full impact of these disparities, but they all highlight possible holes in the system.
In addition to seeking feedback from amputees, I also asked several prosthetists for their opinion of the K-level system. All of them emphasized that they take a holistic approach to evaluating patients, weighing factors that go far beyond K-levels. They assess each patient’s overall health and ask about their lifestyle goals and perceived potential. All stressed the importance of ongoing evaluation and encouraged patients to view their initial K-level as a starting point, not a final destination. Every prosthetist I spoke to believes in the possibility of growth and reassessment, recognizing that a person’s abilities and aspirations can evolve significantly over time.
It’s important to note that K-level assessments aren’t always conducted by the prosthetist. Your K-level may be set by your primary care physician, rehabilitation doctor, or physical therapist. No matter which clinician is doing the evaluation, it’s up to you to advocate for yourself and make them aware of your goals—and continue to do so at every step along the way. If your fitness improves and/or your lifestyle objectives change, you can request a new K-level assessment. (See the sidebar for details about how to do that.) When I select a primary care physician, I always ensure they have experience with amputees and K-levels or are on board with advocating for me.
Toward a New System
The need for change is not just anecdotal; it’s backed by emerging research. Recent studies are pointing the way toward personalized, data-driven methods for assessing amputees’ mobility potential.
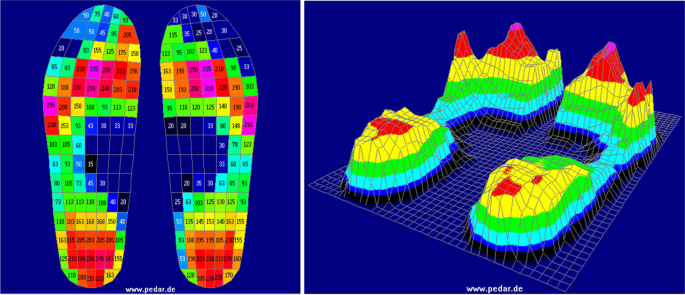
One study, published last summer in Biomedical Engineering Advances, investigated whether wearable sensors that monitor walking cadence could form a quantitative basis for assigning K-levels. By analyzing the data with a machine learning model, the researchers found that stride rhythm and speed are key mobility indicators that correlate closely with K-levels assigned through conventional methods. This exploratory exercise examined whether walking cadence is consistent across patients who’ve lost limbs for varying reasons, addressing an important question about the impact of underlying pathology on gait patterns. For example, as a congenital below-knee amputee I have a unique residual limb anatomy that differs from that of someone with an acquired below-knee amputation, which directly affects my walking speed and cadence. Further research with larger sample sizes could pave the way toward more precise, scientifically validated mobility assessments.
A second study, published last fall in Physical Medicine and Rehabilitation Clinics, emphasized the importance of tailoring mobility assessments to each individual, with deep consideration of their unique circumstances and personal goals. This paper focused on decision-support tools that empower patients to participate actively in their own prosthetic care, helping them communicate effectively with clinicians and contribute meaningfully to decision-making. “Predicting functional outcomes is a critical step in personalizing prosthesis prescrip-tion,” the paper concludes, “ensuring that these decisions align with individual patients’ priorities and preferences.”
So can the K-level system be repaired, or should it be replaced? Those who favor preserving the K0-K4 scale have proposed reforms such as routine reassessments, greater emphasis on long-term aspirations over short-term limitations, and better integration of prosthetist and patient input into the classification process. But many believe the current framework is just too outdated to reflect the way amputees live in the 21st century. They argue that it’s time to eliminate rigid categories in favor of a more dynamic approach that reflects the diversity of amputee lifestyles and prosthetic technologies.
Whether the K-level gets a makeover or is scrapped entirely, any change would require significant buy-in from key stakeholders. In addition to amputees themselves, reform would have to involve Medicare officials, private insurers, prosthetists, rehab clinicians, researchers, and advocacy organizations such as the Amputee Coalition.
The path forward won’t be easy. But the need for change at some level is clear. Amputees aren’t defined by a single moment of assessment. Our present mobility and future potential aren’t static—they evolve with time, effort, and the right support. It’s time for a system that reflects that reality.
How to Get Your K-Level Reclassified
Many amputees don’t realize that K-levels aren’t set in stone. If your abilities have improved, you can request a reassessment—and that, in turn, can help you get covered for a more advanced prosthetic device that keeps you on an upward trajectory.
Here’s a four-step formula to raising your K-level:
- Establish your mobility baseline by gathering medical and rehabilitation records from your previous K-level assessment.
- Work with your prosthetist to document your progress from the baseline. If possible, use objective measures such as walking speed, stride length, and ability to navigate stairs or inclines.
- Share the documentation with your primary care physician and request a new functional assessment to demonstrate your improved mobility potential.
- Appeal if necessary—many amputees successfully challenge initial K-level assignments.







.jpeg)

-1.png "Gaza Fund (1)-1")
.jpg)
