A research studies-based programme is ongoing at present in Sri Lanka to create culturally relevant, sustainable prosthetics for low- or middle-income countries, specifically to co-design and develop new prosthetic devices including new portions of the same that help those with limb loss in Sri Lanka.
This was mentioned in an original article on ‘The legacy of war: Improving lower-limb prosthetic design in Northern Sri Lanka’ which was authored by M.A. Berthaume (attached to England's King's College London's Engineering Department) and Consultant Paediatrician M.G. Sathiadas (also a Senior Lecturer attached to the Jaffna University Faculty of Medicine, Paediatrics Department, and the Editor of the Jaffna Medical Journal) and published in the said Journal's 37th Volume's First Issue, last month.
The internal conflict in Sri Lanka has left a population of amputees, most of whom live in the North and the East, where the conflicts took place. When the war was occurring, and for several years afterward, this attracted the attention of the global humanitarian community, and organisations like the International Committee of the Red Cross (ICRC), Motivation, and Exceed Worldwide provided resources (e.g., training, skilled workers, donations, and consumables) to provide prosthetics to help people live more fulfilled lives. As international aid and donations abated, it fell upon national resources (e.g., the Government, local hospitals and charities) to fill this gap. One such charity is the Jaffna Jaipur Centre for Disability Rehabilitation (JJCDR).
Established in 1987 to help those who lost limbs during the war, the JJCDR has been a regular provider of prosthetic (an artificial body part – a prosthesis), orthotic (artificial support or brace for the limbs or spine), and mobility services to Sri Lankans for over 35 years. Located in Jaffna, most of its patients come from the Jaffna Peninsula, but it has become so renowned for its services that people travel from across the island for JJCDR’s prosthetic services.
The prosthetics currently provided by the JJCDR are local variations of the ICRC’s prosthetic technology. Focused on local manufacture, these prosthetics largely use local materials which increase their durability and longevity in the hot, humid, Sri Lankan environment. However, the ICRC prosthetics were not designed with Sri Lankans in mind. Instead, they were manufactured for functionality, flexibility, and affordability so that they could be used by anyone across the globe.
As part of an ongoing collaboration between the United Kingdom (UK) and Sri Lankan universities, hospitals, and charities, Berthaume et al. undertook two studies to better understand the amputee population in the North and how they were using their lower-limb prosthetic devices. The information from these studies will be used to co-design new portions of the prosthetic devices so that they better serve the biological and cultural anthropological needs of the local amputee population sustainably.
This unique combination of engineering (i.e., design) and anthropology (i.e., culture and biology) is referred to as anthroengineering (M.A. Berthaume and P.A. Kramer's ‘Anthroengineering: An independent interdisciplinary field’, and C.A. Barth, A. Wladis, C. Blake, P. Bhandarkar, S.A. Perone and C. O’Sullivan's ‘Retrospective observational study of the characteristics of persons with amputations accessing ICRC rehabilitation centres in five conflict and post-conflict countries’).
Demographic, medical, and financial stats from the JJCDR (1987-2018):
There were 3,665 unique patients who registered with the JJCDR from 1986-2018. The majority of them were male (2,605), with 1,060 females. More men receive prosthetic and orthotic (P&O) services than women, and this is common around the world. Unsurprisingly, given the large percentage of war-related amputations, most patients were young at the age of amputation, and consequently young when they registered with the JJCDR.
Occupations can change with time, but, of the 555 patients with occupation-related data, 124 were housewives and 85 were unemployed, implying that it would likely be more important to have prosthetics that are efficient at walking down the street and moving about a house, instead of those meant for high, strenuous loads that might be more important to a labourer. Unsurprisingly, most patients lived in the Jaffna Peninsula at the time of registration (82.5%/2,851 out of the 3,455 with address-related information) and most (94.3%/2,382 out of 2,525) lost their limb(s) in the Northern Province.
Most prosthetic patients with the reason for amputation recorded (2,556) had war-related amputations, and had had their amputations done at teaching hospitals (65.6%/2,100 out of 3,202). Most of the amputees were lower-limb amputees, which again is unsurprising as landmines and shell blasts tend to result in lower-limb amputations. The JJCDR also provides limited upper-limb prosthetics, so, it is possible that the upper-limb amputee community in the region is higher, and that they do not receive prosthetic services from the JJCDR.
Potentially, one of the most important findings is the temporal changes in the cause of amputation. Since the conflict has ended, landmine and shell blast amputations have gone down significantly, although landmine amputations do still occasionally occur due to legacy mines. As in many other countries, diabetic (a group of common endocrine diseases characterised by sustained high blood sugar levels, due to either the pancreas not producing enough of the hormone insulin, or the cells of the body becoming unresponsive to insulin's effects) amputations are on the rise: this is unsurprising, given the increase in diabetes within Sri Lanka, and the large percentage of Sri Lankans who have undiagnosed diabetes (S. Amarasinghe, S. Balakumar and V. Arasaratnam's ‘Prevalence and risk factors of diabetes mellitus among adults in the Jaffna District’, and P. Katulanda, G.R. Constantine, J.G. Mahesh, R. Sheriff, R.D.A. Seneviratne, S. Wijeratne, M. Wijesuriya, M.I. McCarthy, A.I. Adler and D.R. Matthews's ‘Prevalence and projections of diabetes and pre-diabetes in adults in Sri Lanka — the Sri Lanka Diabetes, Cardiovascular Study’). As the survival rate for those with diabetic amputation is low (largely due to co-morbidities with the disease progressing), knowledge and treatment of diabetes is critical for the community.
Finally, it became clear that the costs associated with the provision of new prosthetic devices vastly outweighed the costs associated with repairing existing devices. This is important from a design perspective, as it highlights the need for modular prosthetics that can be easily disassembled, repaired, and reassembled quickly and easily (M. Berthaume, S. Barnes, S. Hettiaratchy, J.C. Clasper, A. Kumar, G. Sathiadas and J. Ganeshamoorthy's ‘Demographic, medical, and financial statistics from the JJCDR database, 1987-2018: A prosthetics, orthotics, and mobility clinic in Northern Sri Lanka’).
Mechanical failure of prosthetic feet
Working with the JJCDR, Berthaume et al. collected 122 prosthetic feet (November 2019-July 2022) that were replaced by the JJCDR due to failure. The vast majority (105) were manufactured by the JJCDR, using either fibre-reinforced nylon coated rubber (66, referred to as ‘string rubber’) or non-fibre-reinforced nylon (34, referred to as ‘sheet rubber’). Five prosthetic feet were worn past the point of identification as string or sheet.
The prosthetic feet are the soft ankle cushion heel (SACH) design created by the ICRC. The SACH foot manufactured at the JJCDR consists of three main components: a hard, polypropylene (plastic) keel surrounded by natural rubber, with a nylon layer at the bottom. The keels, manufactured by the JJCDR, are all the same size, meaning that the distal end of the keel is closer to the toes in the smaller feet, and relatively closer to the heel in the larger feet. The keel is an important component of the SACH foot, as it provides structural integrity, and allows the prosthetic foot to connect to the ankle component. The rubber acts as a damper and energy storage unit, making it easier for the amputee to walk, and making gait less jarring.
Unlike what would be predicted under the ISO 10328 standards (Prosthetics – Structural testing of lower-limb prostheses – Requirements and test methods) for the design and testing of safe lower-limb prosthetics, Berthaume et al. found little evidence of the prosthetic feet fracturing. Berthaume et al. were unable to decisively determine if the delamination (separation of a material into its constituent layers) between the keel and the rubber occurred without cutting into the feet, but, it was clear from some feet that the keel was moving around freely within the rubber, meaning that delamination had occurred.
In terms of why the feet were replaced, the most common reason given by the people who worked at the JJCDR was wear on the bottom of the feet. Essentially, the prosthetic foot would start to wear at the heel and the distal end of the keel. When this happened, the keel would start to delaminate from the rubber and push through the bottom of the foot. The keel would then wear away as it rubbed the ground, lessening the structural integrity of the foot and eventually causing the foot to fracture, which could cause the prosthetic user to fall and become injured. The feet were therefore replaced when the feet were worn, but before the keel pushed through the bottom of the foot.
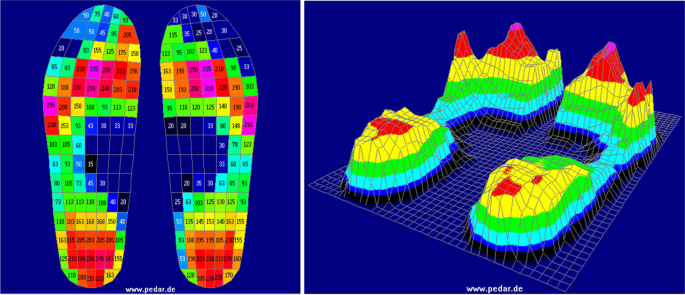
To quantify how the feet were wearing, Berthaume et al. developed a qualitative method derived from the study of tooth wear. Pictures of the soles of the feet were taken, and a 20 by 10 grid was placed on top of it. Each square was assigned a score from zero to nine, with zero implying that the foot was newly manufactured and not yet used, and nine implying that the portion of the foot was completely missing (e.g., a big toe had broken off).
The average (a number expressing the central or typical value in a set of data, in particular the mode [the value that occurs most frequently in a given set of data], median [denoting or relating to a value or quantity lying at the midpoint of a frequency distribution of observed values or quantities, such that there is an equal probability of falling above or below it], or, most commonly, the mean [the value obtained by dividing the sum of several quantities by their number - an average], which is calculated by dividing the sum of the values in the set by their number), standard deviation (a quantity expressing by how much the members of a group differ from the mean value for the group), and coefficient (a numerical or constant quantity placed before and multiplying the variable in an algebraic expression) delamination of the variation were calculated for each square across the 66 feet. It was found that, as predicted by those working at the JJCDR, on average, the distal end of the keel and the perimeter of the foot were more worn than other portions of the foot.
These areas should be structurally reinforced to increase prosthetic foot longevity. Berthaume et al. also hypothesised that the standard deviation and coefficient of the variation may capture differences in behaviour and locomotor biomechanics between individuals.
This data helped create a biomechanical model for understanding how these prosthetic feet fail. When walking, the prosthetic user places the heel of their foot against the ground (i.e., the heel strike phase of locomotion). The amputee then shifts their centre of gravity over the prosthetic foot during the mid-stance phase, eventually lifting the heel of the prosthetic foot off the ground (heel off). When this occurs, the rigid portion of the foot, with the keel, remains fairly stable, but, the distal end of the foot bends much like a foot bends around the metatarsophalangeal joint (the joint of the foot located between the long bones of the mid-foot and the bones of the toes, and which joint is crucial for proper foot function, particularly during walking and weight-bearing activities) in an intact foot, putting bending moments and large pressures about the distal end of the keel. During the toe off, this portion of the foot is rubbed against the ground, causing wear.
One of the big implications of this study is the understanding of how to design prosthetic feet for non-European countries. In countries like the UK, prosthetic feet must pass the ISO 10328 tests before being sold on the open market. These tests put foot prototypes through a series of mechanical tests (static and dynamic loads), and factors like deformation, delamination, and fracture and investigated to determine if the product is ready for the market. Unfortunately, the ISO 10328 tests do not consider factors like foot wear, likely because prosthetic wear is not a factor that needs considering in the countries which sent representatives to help develop the ISO 10328 standards.
In Sri Lanka, there is a culture of wearing open-toed shoes, like sandals, and walking barefoot. This causes the prosthetic feet to wear faster than if they were worn with closed-toed shoes, making wear an important factor in prosthetic feet failing and needing to be replaced. Thus, foot wear, which is not considered by the ISO 10328 tests, must be considered when designing prosthetic feet for countries like Sri Lanka (G. Ranson, M. Morley, N. Corsial, G. Sathiadas, J. Ganeshamoorthy and M. Berthaume's ‘The mechanical failure of locally manufactured prosthetic feet from the JJCDR’).







.jpeg)

-1.png "Gaza Fund (1)-1")