
When you wake up from amputation surgery, the clock is already ticking. How quickly you get the right wound care, when you first get out of bed, whether you receive proper rehabilitation, and other post-operative decisions can influence how long you’ll be in the hospital, the difficulty of your rehab process, and the odds that you’ll regain the ability to walk.
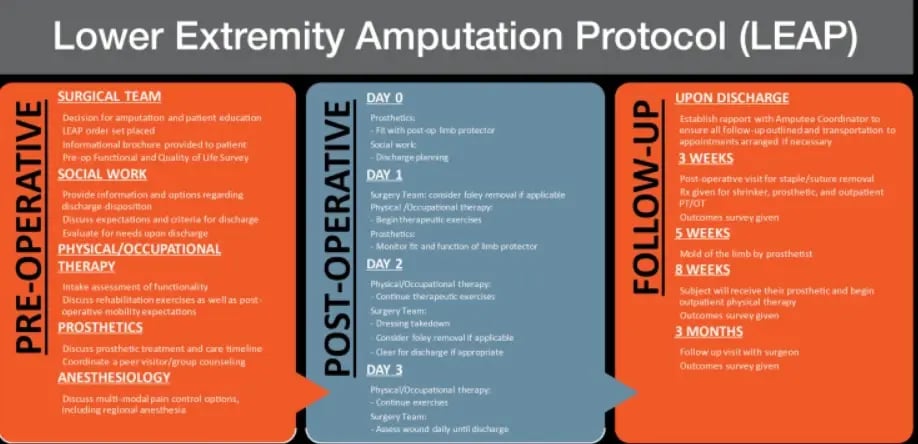
The Lower Extremity Amputation Protocol (LEAP) provides a clear roadmap for healthcare providers. Multiple small-scale studies have shown that when hospitals follow LEAP—which covers everything from wound care to PT, OT, pain management, prosthetic care, peer guidance, mental health, and beyond—their amputee patients have much better health outcomes.
Unfortunately, most hospitals still aren’t following LEAP. To understand why, a pair of Columbia University researchers surveyed the doctors, nurses, and other healthcare providers who provide post-amputation care at a major urban teaching hospital. They sent a detailed questionnaire to 389 clinicians involved in all aspects of amputee care. Nearly 250 clinicians (61 percent) responded, and their feedback was sobering. An overwhelming 93 percent of respondents weren’t familiar with the clinical practice guidelines for amputation rehabilitation. About 60 percent weren’t even familiar with the common problems that delay hospital discharge after amputation.
When it came to specific post-amputation practices, the numbers were even more concerning. While most clinicians had some familiarity with soft dressings (the basic technique for wrapping a residual limb immediately after amputation), nearly half were unfamiliar with semirigid or rigid dressings—the more advanced techniques that research shows work better. And almost 90 percent of non-prosthetist clinicians had no experience using temporary prostheses to help patients start working toward ambulation before they’ve been fitted for a prosthesis.
Most of the respondents acknowledged that their skills fell short and wanted to provide better post-amputation care. They were eager to learn about and adopt evidence-based practices; they just hadn’t been taught. And while time constraints often pose a barrier in modern healthcare, clinicians didn’t identify this as a major obstacle to implementing better amputation care protocols. Instead, the researchers identified 12 major barriers, which fell under two main headings: capability and opportunity.
The capability barriers were straightforward: Clinicians lacked the knowledge, skills, and hands-on experience needed to provide specialized amputation care. Even with the rapid growth in vascular amputee cases, amputations are relatively rare compared to procedures related to heart disease, cancer, and other common conditions. About two-thirds of respondents (excluding prosthetists) had seen fewer than five amputee patients in the past year. Bottom line, many clinicians simply don’t encounter enough cases to build expertise. Between 85 and 90 percent of respondents said they lacked confidence in multiple aspects of post-amputee care.
The opportunity barriers were more systemic. Even well-trained, confident clinicians struggled within an environment that didn’t support coordinated amputation care. Communication between surgery teams and rehabilitation specialists was a major issue—86 percent identified it as a barrier. Interdisciplinary coordination scored 82 percent; getting timely prosthetic support, 86 percent; lack of administrative directives or institutional guidelines, 84 percent.
These responses reinforce the fact that post-amputation care doesn’t function well when it’s siloed. It requires integration and teamwork among surgeons, nurses, therapists, and prosthetists. But in a large teaching hospital with constantly rotating staff, building that coordination is extremely difficult. “Hierarchical healthcare culture emphasizes physician knowledge, yet staff rotations mean cycles of training and relationship-building that challenge consistent practice and communication,” the researchers note.
Based on their findings, the authors proposed four strategic interventions, each addressing specific barriers:
1. Accessible Education: Create short, multimedia clinical practice resources available on-demand via the hospital network. Clinicians need to access evidence-based information quickly, right when they need it.
2. Hands-On Training: Schedule regular training sessions that account for hospital rotations. Because staff rotate through different services, one-time training isn’t enough. Regular, repeated, hands-on education helps new clinicians get up to speed and experienced ones stay sharp.
3. Champion Mentorship: Recruit expert clinicians who can provide clinical support, answer questions, and model best practices for their colleagues. These champions would serve as go-to resources for teams learning new techniques.
4. Automated Order Sets: A standardized, automated multidisciplinary referral system emerged as perhaps the most crucial intervention. When a patient undergoes amputation, the system would automatically trigger all necessary consultations and interventions, without requiring individual clinicians to remember every step.
This research served as a reminder that shortfalls in amputee care aren’t intractable, and they don’t occur because clinicians don’t care or because the science is unclear. They occur because the gap between what we know works and what actually happens involves dozens of overlapping barriers—from individual knowledge gaps to institutional systems to communication challenges. “While the ultimate goal is improving patient-level outcomes such as earlier mobility milestones, shorter hospital lengths-of-stay, and faster prosthetic fitting,” the researchers conclude, “this study targeted provider- and organization-level behaviors.”
The paper, “Implementation of an evidence‑based multidisciplinary post‑operative lower extremity amputation protocol (LEAP),” is available online at Implementation Science Communications. For a detailed discussion of LEAP’s specific guidelines, see the August 2022 edition of Journal of Vascular Surgery Cases, Innovations and Techniques.














