Functional classification plays a central role in prosthetic prescription. The K-level system, widely used in prosthetic rehabilitation, was introduced to help clinicians match prosthetic technology to a patient’s expected mobility level. While the framework remains a key tool in clinical practice, its influence on patient care, reimbursement and device selection continues to generate discussion within the orthotics and prosthetics profession.
Original article:
https://opedge.com/k-levels-in-practice-the-impact-on-patient-care/
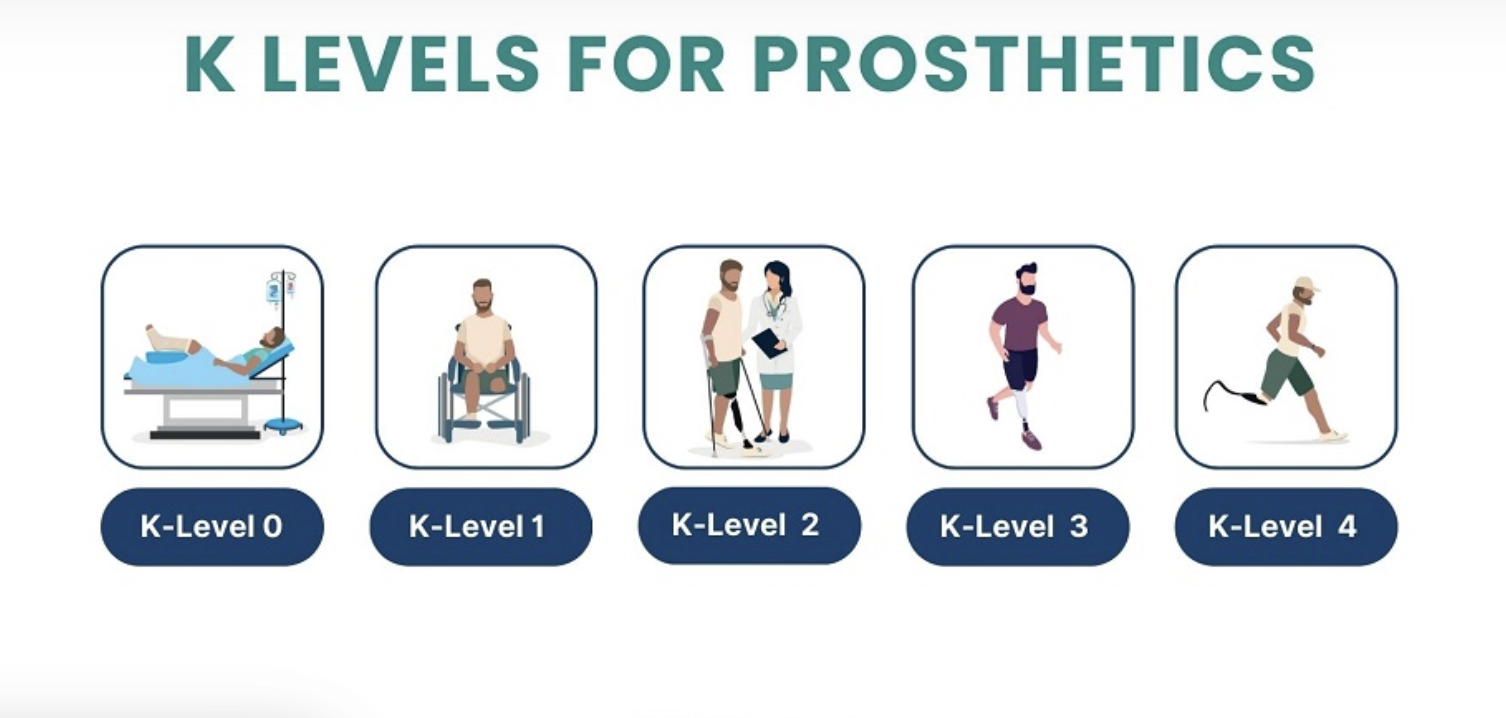
What Are K-Levels?
The K-level system was introduced in 1995 by the Centers for Medicare & Medicaid Services (CMS) to classify the functional mobility of individuals with lower-limb amputations. The scale ranges from K0 to K4, representing mobility levels from non-ambulatory individuals to highly active users capable of high-impact activities.
The goal of the system is straightforward: match patients with prosthetic components that are appropriate for their functional potential. Before the system was implemented, prosthetic technology prescriptions were often inconsistent, with some patients receiving devices that were either too advanced or insufficient for their mobility needs.
How K-Levels Influence Clinical Decisions
Today, K-levels influence multiple aspects of prosthetic care. They guide clinicians when selecting components, help manufacturers design products for specific activity levels and serve as a key factor in reimbursement decisions by insurers.
In practice, the classification system shapes the entire prosthetic ecosystem—from how devices are developed to how clinicians structure treatment plans.
However, while K-levels provide a useful framework, their application is not always straightforward.
The Challenge of Predicting Patient Potential
One of the most difficult aspects of the K-level system is predicting a patient’s future mobility. Assessments can accurately measure a patient’s current functional capacity, but predicting long-term potential is far more complex.
Experts note that a person’s mobility six months after evaluation may differ significantly from their initial assessment. Recovery speed, comorbidities, training opportunities and motivation can all influence outcomes.
As a result, clinicians must often combine formal assessment tools with clinical judgement when determining the most appropriate classification.
When Prescription and Mobility Do Not Align
Research suggests that prosthetic prescriptions do not always match a patient’s functional level. In some cases, devices are underprescribed, limiting a patient’s ability to reach their mobility potential. In others, components may be overprescribed, providing more advanced technology than the patient can effectively use.
Several factors can contribute to these mismatches, including:
- variations in rehabilitation progress
- differences in clinician experience
- payer reimbursement restrictions
- inconsistent use of outcome measures
These challenges highlight the importance of comprehensive evaluation and ongoing reassessment throughout the rehabilitation process.
Using Objective Assessment Tools
To improve accuracy in functional classification, clinicians often rely on validated outcome measures. One widely used example is the Amputee Mobility Predictor (AMP) assessment, which helps evaluate mobility capabilities and supports K-level determination.
Tools like the AMP provide objective data to support clinical judgement and improve consistency when assigning functional levels.
However, no single assessment can fully predict long-term patient outcomes. For this reason, clinicians must interpret test results within the broader context of the patient’s medical condition, rehabilitation goals and lifestyle.
Looking Beyond the Classification System
Although the K-level system remains central to prosthetic care, some experts believe that future approaches may move toward more sophisticated predictive models.
Advances in data analytics and outcome measurement may allow clinicians to analyse large patient datasets to better estimate mobility potential. Factors such as age, cause of amputation, comorbidities and rehabilitation progress could be incorporated into predictive tools that support more personalised prosthetic prescriptions.
Such approaches could help clinicians make more informed decisions about component selection and rehabilitation planning.
Balancing Frameworks with Individual Care
Despite its limitations, the K-level system continues to provide an important framework for prosthetic prescription. It offers a common language for clinicians, payers and manufacturers while helping guide technology selection.
However, effective prosthetic care requires more than classification alone. Clinical expertise, patient goals and rehabilitation progress all play critical roles in determining the most appropriate device for each individual.
Ultimately, the challenge for prosthetists is to use the K-level system as a guideline rather than a rigid rule, ensuring that patients receive prosthetic solutions that support both their current abilities and their long-term mobility potential.