.jpg)
As prosthetists, we know that liners serve as the immediate interface between the residual limb and the socket—yet, compared to sockets themselves, liner parameters like thickness are less frequently studied in depth. A recent computational modeling study published in Nature Scientific Reports shines light on how modest adjustments in liner thickness (on the order of just a few millimeters) may meaningfully influence pressure, shear, strain, and limb displacement.
Here’s a breakdown of their methodology, findings, and clinical take-aways:
Study Overview & Methodology
-
The researchers constructed an anatomically accurate 3D model of a transfemoral residual limb (using CT and MRI to capture bone, muscle, and nerve architecture).
-
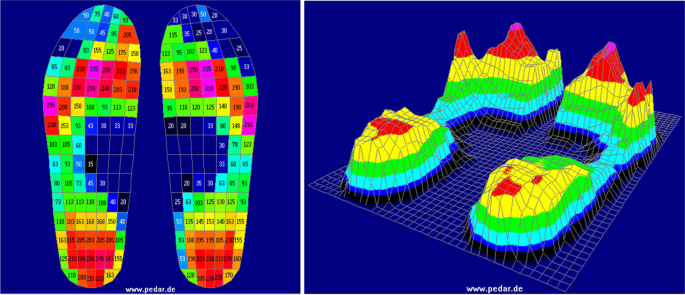
They simulated a socket and liner system, using finite element modeling (FEM) to analyze stress, strain, and motion under load.
-
Two common liner materials—gel and silicone—were tested at three thickness levels: 2 mm, 4 mm, and 6 mm.
-
Key metrics included:
Key Findings & Interpretation
1. Thicker Liners → Lower Pressure & Shear, But Increased Displacement
-
Pressure: For gel liners, the model showed that a 6 mm liner reduced peak pressures by ~18% compared to a 2 mm liner. For silicone, the drop was even more notable (over 50% difference between 2 mm and 6 mm).
-
Shear and Strain: Gel liners—especially thinner ones—exhibited higher shear stresses and more concentrated strain “hot spots.” Silicone liners, at all thicknesses tested, produced lower peak stress and more evenly distributed strain patterns.
-
Displacement (Micro-motion): As liner thickness increased, the residual limb experienced more vertical displacement (i.e., increased “slippage” within the socket). This effect was more pronounced for silicone than for gel in the model.
2. Trade-Offs Are Inevitable
-
Thicker liners help to mitigate pressure, shear, strain—all of which helps reduce risk of skin breakdown, discomfort, and nerve irritation.
-
But greater micro-motion may compromise stability, alter gait dynamics, risk pistoning, or reduce patient confidence.
-
Silicone offers better stress and strain handling, but gel may provide more mechanical coupling (i.e., stability) in some contexts.
Clinical Considerations & Suggestions for Practice
Even though this study is purely computational and lacks in vivo validation, it offers a framework to inform liner choices. Here are some prosthetist-level considerations:
| Clinical Factor | Relevance | Practical Application |
|---|---|---|
| Patient tissue quality | Fragile skin, scarred or sensitive residual limbs may benefit from thicker liners that reduce peak stresses | Consider a thicker liner (e.g. 5–6 mm) especially in higher-risk cases |
| Stability & gait goals | For more active patients requiring tight coupling, micro-motion must be minimized | A slightly thinner liner (balanced with proper suspension and socket fit) may preserve control |
| Material selection | Silicone models show lower stress and strain in simulation | Use silicone liners especially in cases where tissue protection is a priority |
| Socket fit & alignment | Excessive micro-motion can degrade interface repeatability | Reassess socket fit and suspension if increased displacement is observed clinically |
| Patient feedback & symptoms | Complaints of hotspots, irritation, or looseness should prompt evaluation of liner properties | Use this data as a conversational point with patients during fitting/tuning |
Caveats & Future Directions
-
The findings are model-based, not yet validated by clinical trials or long-term patient data. Real human anatomy, tissue heterogeneity, and dynamic behavior may deviate from models.
-
The model did not explicitly account for all variables (e.g. sweating, liner aging, daily volume fluctuations, shear from dynamic gait cycles).
-
A future step would be a clinical study correlating liner thickness/material to outcomes—e.g. skin health, patient comfort, gait metrics, and residual limb volume change over time.
Clinical Guidelines: Prosthetic Liner Thickness and Patient Comfort
Purpose
To guide prosthetists in selecting prosthetic liner thickness and material to optimize comfort, tissue protection, and socket stability.
1. Patient Assessment
-
Skin & Tissue Quality
-
Fragile, scarred, or sensitive skin → prioritize thicker liners (5–6 mm).
-
Robust tissue with good tolerance → thinner liners may be considered for improved control.
-
-
Residual Limb Shape & Volume
-
Conical or irregular limbs may benefit from added cushioning.
-
Volume fluctuation patients may require adjustable suspension in addition to liner thickness considerations.
-
2. Liner Thickness Selection
-
Thin Liners (2–3 mm)
-
Indicated for: high-activity patients, those needing maximal stability and limb-socket coupling.
-
Risks: higher peak pressures and shear, increased skin irritation potential.
-
-
Medium Liners (4 mm)
-
Balanced option for general use, providing both cushioning and reasonable stability.
-
-
Thick Liners (5–6 mm)
-
Indicated for: patients with sensitive tissue, history of skin breakdown, or nerve pain.
-
Risks: increased vertical displacement (micro-motion), potential gait instability, pistoning.
-
3. Material Considerations
-
Silicone Liners
-
Lower stress and strain concentrations.
-
Better tissue protection.
-
Slightly more displacement risk with increased thickness.
-
-
Gel Liners
-
Higher shear stresses but better limb stability (less displacement).
-
May be preferable for patients prioritizing control over cushioning.
-
4. Clinical Trade-Offs
-
Thicker liners reduce stress and strain but may increase micro-motion.
-
Thinner liners enhance stability and control but elevate pressure and shear risk.
-
Always balance comfort vs. control according to patient activity level and tissue health.
5. Fitting & Follow-Up
-
Reassess socket fit when altering liner thickness.
-
Monitor for:
-
Hotspots or redness (pressure/shear).
-
Looseness or pistoning (micro-motion).
-
Patient-reported comfort and functional confidence.
-
-
Adjust suspension or alignment if displacement increases with thicker liners.
6. Clinical Documentation
-
Record liner type, thickness, and rationale in patient file.
-
Track patient outcomes (comfort, skin health, gait stability) for ongoing evaluation.
To read the full paper, log on at Nature Scientific Reports.







.jpeg)

-1.png "Gaza Fund (1)-1")